MUSCLE3X
Exercise Pain and Recovery Kit
Exercise Pain and Recovery Kit
Couldn't load pickup availability
Many dietary supplements are marketed to athletes for purposes that extend beyond the classic ergogenic aid definitions. Examples include supplements that help to reduce exercise-induced pain & inflammation and improve recovery.
During and especially after athletic activity, the body has a number of responses in order to help it recover and adapt. Many of these responses involve some level of local inflammation and muscle soreness that peaks within 24 to 48 hours after the exercise, usually referred to collectively as delayed onset muscle soreness (DOMS). These processes may contribute to various functional deficits such as reduced strength and/or range of motion. (Davis 2007)
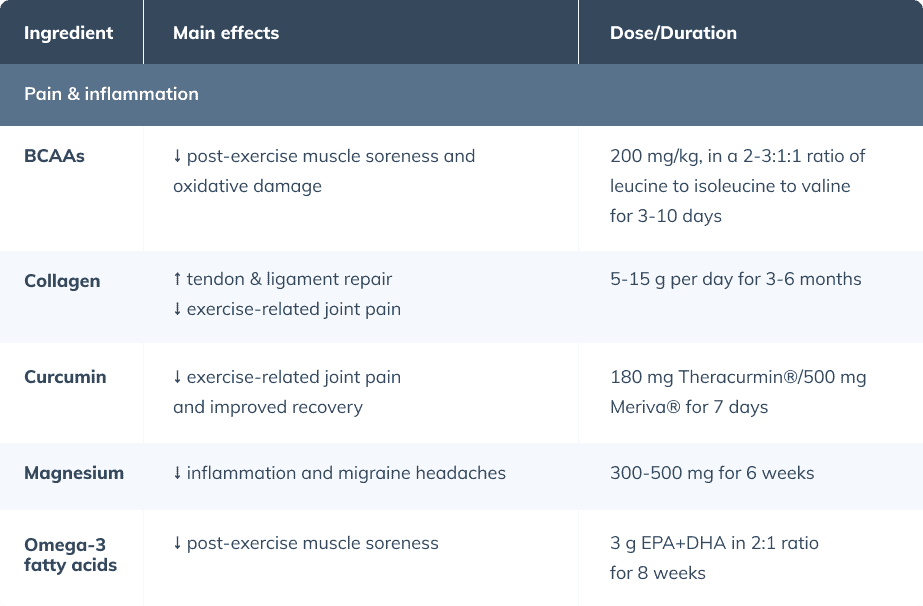
The ingredients selected for this protocol may help improve symptoms of exercise-related pain and aid in recovery. For example, branched-chain amino acids (BCAAs) may provide extra quantities of certain amino acids that may help to reduce markers of exercise-related damage. (Khemtong 2021) Collagen acts to provide strength and elasticity to connective tissues. (Dressler 2018) Curcumin reduces many inflammatory markers and may shorten recovery time from exercise. (Fang 2020)(Suhett 2021) Magnesium may reduce inflammation and cortisol levels and improve immunological function, all aiding in recovery. Finally, omega-3 fatty acids have effects on cyclooxygenase-2 expression and the metabolism of arachidonic acid. (Ochi 2018)
BCAAs
Branched-chain amino acids (BCAAs)
~200 mg/kg/day (i.e., 14 g for a 70 kg individual) for 3-10 days (Fouré 2017)
2-3:1:1 ratio of leucine:isoleucine:valine (Salinas-Garcia 2014)
- BCAAs include the three essential amino acids leucine, isoleucine, and valine. BCAAs and especially leucine have been reported to activate mTOR, thereby promoting muscle protein synthesis, (Fouré 2017) though there is controversy around these claims. (Wolfe 2017)(Churchward-Venne 2014) BCAAs have been postulated to improve recovery since they have been shown to reduce markers of oxidative damage and muscle soreness.
- A 2017 systematic review found that BCAA supplementation may reduce skeletal muscle damage markers when muscle damage was low-to-moderate, the BCAA daily intake was high (over 200 mg per kilogram body weight) and prolonged (greater than ten days), and the BCAAs were taken prior to exercise. (Fouré 2017)
- A 2021 meta-analysis showed that BCAA supplementation reduced creatinine kinase levels, but not plasma lactate dehydrogenase, two markers indicative of muscle damage and soreness, after resistance exercise in trained males. (Khemtong 2021)
- BCAAs may reduce delayed-onset muscle soreness with a moderate effect (effect size = 0.73), particularly within 48 hours post-exercise, according to a 2019 meta-analysis. (Fedewa 2019)
- No adverse effects of BCAA supplementation were noted, (Fouré 2017)(Wolfe 2017) which is consistent with the fact that BCAAs are simply a small source of protein in the diet.
Collagen
Collagen
5 to 15 g per day for 3 months. (Clark 2008)(Zdzieblik 2017)(Dressler 2018)(Praet 2019)(Shaw 2017)
- Collagen is responsible for elasticity and firmness of tendons, ligaments, and connective tissues, and comprises one of the most predominant components of the extracellular matrix. The ankle joint as an example is 70% collagen. During supplementation, a considerable proportion accumulates in tissue structures, and may stimulate extracellular matrix expression and biosynthesis within connective tissues. (Dressler 2018)
- Collagen may improve activity-related joint pain compared with placebo when ingesting 5 to 10 g per day over 12 to 24 weeks in young athletes with functional knee issues. (Clark 2008)(Zdzieblik 2017)
- Tendon and ligament repair may be improved with collagen supplementation; 100 athletes with chronic ankle instability were given 5 to 15 g of collagen per day over three to six months. Mechanical stability (measured by ankle stiffness with an ankle anthropometer) significantly improved, and the number of ankle sprains at 6-month follow-ups was reduced. (Dressler 2018)
- In addition to aiding in joint pain and tissue repair, collagen may also help to fuel other metrics of recovery, as it was as effective for restoring different strength metrics between sessions of resistance and aerobic exercise. (Rindom 2016)
Curcumin
Curcumin
180 mg Theracurmin®/500 mg Meriva® for 7 days (Suhett 2021)
- Curcumin may improve athletic performance by reducing inflammation, (Davis 2007) supporting mitochondrial biogenesis, (Hamidie 2015), and reducing oxidative stress. (Kawanishi 2013)
- Two recent systematic reviews showed that curcumin reduced inflammatory markers (TNF-ɑ, IL-6, IL-8, and IL-10), decreased pain and muscle damage (creatinine kinase levels), and led to superior recovery and muscle performance (i.e., quicker reduction of DOMS scores and subsequent restoration of muscle strength) in athletes. (Fang 2020)(Suhett 2021)
- Dosing for curcumin supplementation for athletes varies widely based on the specific product extracts, ranging from 180 mg per day of Theracurmin® to 500 mg per day of Meriva®, to 6,000 mg of less common formulations. (Suhett 2021)
- Curcumin is recognized by the U.S. Food and Drug Administration as “Generally Recognized as Safe.” (Gupta 2013) A 2016 meta-analysis examined the use of curcumin supplementation for pain relief and reported the following side effects in eight randomized controlled trials: gastrointestinal disturbances (dyspepsia, abdominal pain/distention, nausea/vomiting, loose stool), fever, pitting edema, and throat infection. All side effects were reported as mild, and none were responsible for withdrawal from the studies. (Sahebkar 2016)
Magnesium
Magnesium
300 to 500 mg per day for 7 weeks (Heffernan 2019)
- Magnesium is an essential micronutrient and a cofactor for over 325 enzymatic reactions involved in cellular metabolism. (Newhouse 2000) It has important roles in protein synthesis, cellular energy production and storage, and cell growth and reproduction. (NIH 2015)(Volpe 2015) Due to these roles, it has been proposed that magnesium may improve fitness in athletes.
- Athletes may be at greater risk of magnesium deficiency. Approximately 60% of athletes were reported to consume less magnesium than the estimated average requirement, (Wierniuk 2013) compared to about 20% of the general population averages, (DiNicolantonio 2018) which may be a result of magnesium depletions associated with higher intensity exercise. (Molina-López, 2012)
- Overall, the benefits of magnesium supplementation for athletes yields mixed results. However, a 2019 systematic review found beneficial effects of magnesium supplementation on strength measures (e.g., standing long jump and one-repetition maximums) and exercise-induced inflammation, DNA damage, cortisol, and immunological blood markers when provided in doses of 300 to 500 mg per day. (Heffernan 2019)
- Magnesium has been examined in non-athletes for other pain- and inflammatory-related conditions such as muscle cramps and migraine headaches. Magnesium supplementation has been shown to effectively reduce migraine intensity and frequency. (Veronese 2020) The evidence for prophylactic magnesium supplementation for leg cramps is weak, (Garrison 2012) though the studied populations were primarily older adults and pregnant women, so further research in athletes is warranted.
- Adverse effects of magnesium supplementation are not commonly noted in research; (Newhouse 2000) however, the Lowest Observed Adverse Effect Level set by the Institute of Medicine for magnesium supplementation is 360 mg per day. Doses at or above this dose were noted to potentially contribute to diarrhea via an osmotic effect. (IOM 1997)
Omega-3 fatty acids
Omega-3 fatty acids (EPA/DHA)
3 g of EPA+DHA in 2:1 ratio for 8 weeks (Ochi 2018)
- EPA may have anti-inflammatory effects through inhibition of cyclooxygenase-2 expression and metabolism of arachidonic acid. (Calder 2017) EPA and DHA are precursors to the ‘5-series’ leukotrienes, protectins, and maresins, each of which possess unique anti-inflammatory actions. (Calder 2017)
- EPA and DHA might decrease post-exercise muscle soreness and improve range of motion. A systematic review noted a reduction of DOMS in six of 12 trials and a lessened range of motion deficit after exercise in three of five trials. They also found interesting findings worthy of further exploration: lessened muscle strength deficit after exercise in two of six trials and a reduction of swelling in the muscle in one of five trials. Results were mixed but generally found no effect on MPS. (Ochi 2018)
- A 2020 review found that trials with positive outcomes such as improved recovery, reduced injury risk, and reduced illness risk tended to have a dose of over 2 g EPA+DHA, a duration over eight weeks, and study populations of untrained (vs. trained) participants. (Thielecke 2020)
- A 2020 systematic review of studies in athletes also showed that four out of the five included RCTs demonstrated consistent benefit of fish oil supplementation for reducing the inflammatory markers IL-6 and TNF-ɑ, muscle soreness, and creatine kinase levels. (Thielecke 2020)
- Supplementary n-3 fatty acids appear to have a low risk of adverse effects, as only one of five randomized controlled trials in a systematic review (Lewis 2020) reported adverse effects, noting poor palatability, gastrointestinal distress, and nausea in 10% of participants. (Oliver 2016) High n-3 consumption may prolong bleeding time; (Meydani 1991) however, the FDA has recognized that intakes of up to 3 g per day of omega-3 fatty acids is generally recognized as safe in humans, even with regards to claims on bleeding tendencies. (US FDA 2004)
Share